
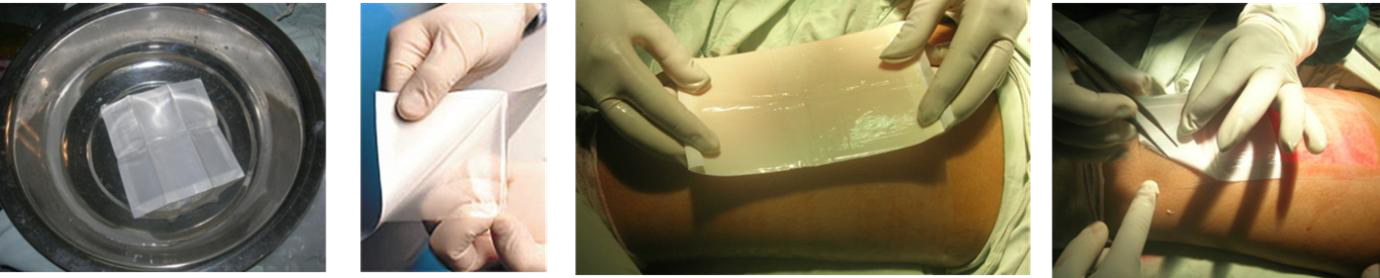




Helicoll® Product Brochure & IFU

Helicoll® Technical and Clinical Info 2024

Helicoll® Innovative Technology, Design, Features, & Benefits

Helicoll® comparison with other FDA cleared products

Helicoll® Clinical Studies and Evidence of benefits
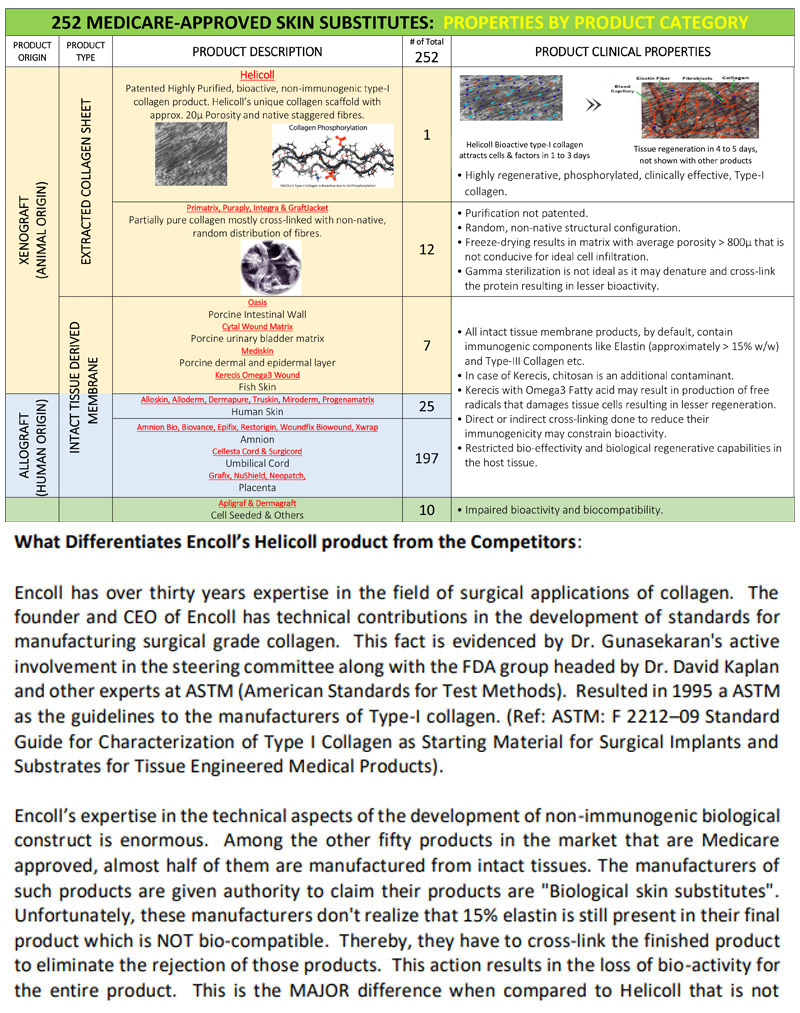
Helicoll® Compared to other Products

Helicoll® Product Details

Helicoll® Unique Features

Helicoll® White Paper on DFU

Helicoll® White Paper on Elastin Carcinogenicity

Helicoll® White Paper on NPWT

Helicoll® White Paper on Tissue Regen Bioactivity

Medical Billing Guide – Medicare
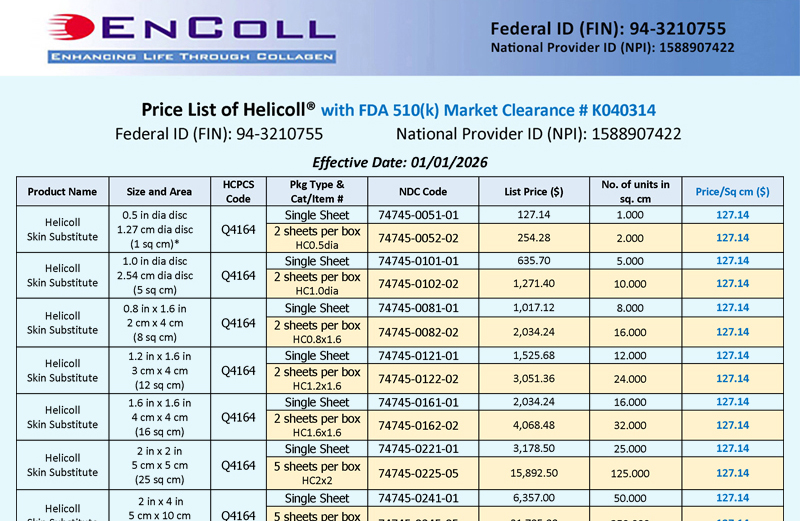
Helicoll® Product Price Catalog
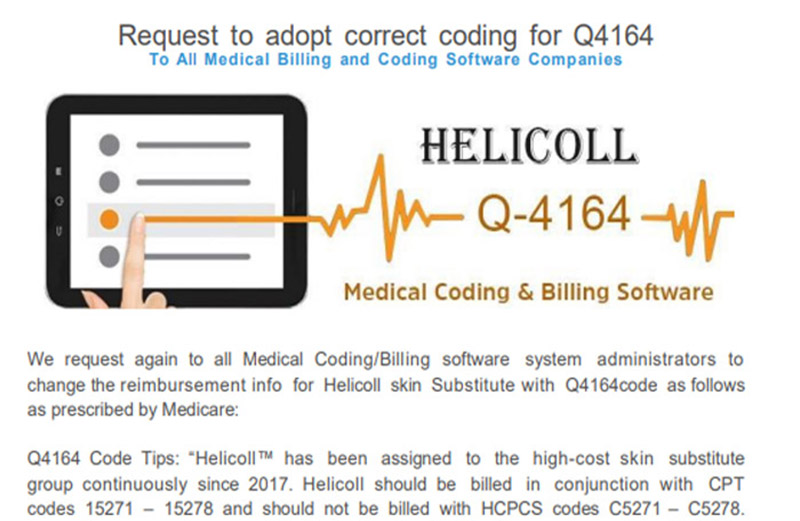
Medicare Recognized Helicoll as a High-Cost skin substitute since 2017
Helicoll Dossier Technical Data
with Cost Calculation

Published Cost Efficiency of Helicoll

For Medical Necessity Sample Letter
Jurisdiction E - Medicare Part B
Skin Substitutes Grafts/Cellular Tissue-Based Products for the Treatment of Diabetic Foot Ulcers and Venous Leg Ulcers Open Public Meeting - May 16, 2024
Comments by the President, Encoll Corp 
Helicoll® FDA 510(k) Clearance

Encoll FDA Mfg License Facility Regn

Helicoll Medicare
Skin Substitute Approval

Helicoll® Trademark Registration

Small Business Certification Cert. No. 2024055

City of Fremont - Business License Certificate
